BPC-157 and TB-500 Together: Evidence, Claims, and What’s Still Speculative
An evidence-aware guide to why BPC-157 and TB-500 are often discussed together, what mechanisms are claimed, what evidence exists separately versus as a combination, and where online recovery claims outrun the data.
BPC-157 and TB-500 Together: Evidence, Claims, and What’s Still Speculative
BPC-157 and TB-500 are often searched together because both are discussed online as “recovery peptides,” but the combination is much less established than the separate mechanism stories suggest. BPC-157 is usually framed around tissue repair, gut protection, tendon and ligament models, angiogenesis, and inflammation-related recovery. TB-500 is usually framed through thymosin beta-4 biology: cell migration, actin dynamics, wound-healing signaling, angiogenesis, and tissue remodeling.
That overlap makes the combination sound logical. It does not make it proven.
The evidence-aware answer is simple: BPC-157 and TB-500 each have preclinical and mechanistic research stories, but strong human evidence for using them together is limited. Most online claims about the pair are built from extrapolation: separate findings, related pathways, anecdotal reports, clinic marketing, and the assumption that two “repair” stories must add up to a stronger result.
This article explains why people pair BPC-157 and TB-500 in searches, what mechanisms are usually claimed, what evidence exists separately versus together, and where the internet gets too confident.
Educational note: This article is for general information only. It is not medical advice, treatment guidance, dosing guidance, sourcing guidance, purchasing guidance, or a recommendation to use BPC-157, TB-500, or any peptide combination.
 The key distinction is separate evidence versus combination evidence. A plausible overlap does not automatically prove the combined use case.
The key distinction is separate evidence versus combination evidence. A plausible overlap does not automatically prove the combined use case.
Quick answer: is there strong evidence for BPC-157 and TB-500 together?
No strong public evidence base establishes BPC-157 and TB-500 together as a proven combination for human recovery, injury healing, tendon repair, muscle repair, or general tissue healing.
A more accurate summary is:
- BPC-157: interesting preclinical repair and protection signals, but limited mature human clinical evidence for common recovery claims.
- TB-500 / thymosin beta-4 discussion: biologically plausible repair-related pathways, but marketed TB-500 claims often lean heavily on broader thymosin beta-4 literature and extrapolation.
- Together: commonly discussed online, but combination-specific evidence is thin compared with the confidence of many claims.
That does not mean the topic is nonsense. It means the responsible question is not “what is the stack?” but “what evidence is being combined, and where does the combination claim outrun the data?”
Why people search BPC-157 and TB-500 together
People usually search for BPC-157 and TB-500 together because both compounds sit inside the same online recovery cluster. Search behavior often comes from a practical question: if one peptide is associated with healing and another is associated with repair, would using both cover more pathways?
The common search intent usually includes:
- tendon, ligament, or soft-tissue recovery claims
- workout injury or sports recovery discussions
- post-injury inflammation and tissue remodeling questions
- “which is better” or “can they be combined” comparisons
- forum anecdotes about pairing the two
- clinic or vendor content implying complementary effects
That logic is understandable. If BPC-157 is described as more “localized repair and protection” and TB-500 is described as more “systemic soft-tissue remodeling,” the pairing sounds tidy. Unfortunately, biology does not care that a marketing table looks symmetrical.
A clean mechanism story can be useful for hypothesis generation. It cannot replace controlled outcome evidence.
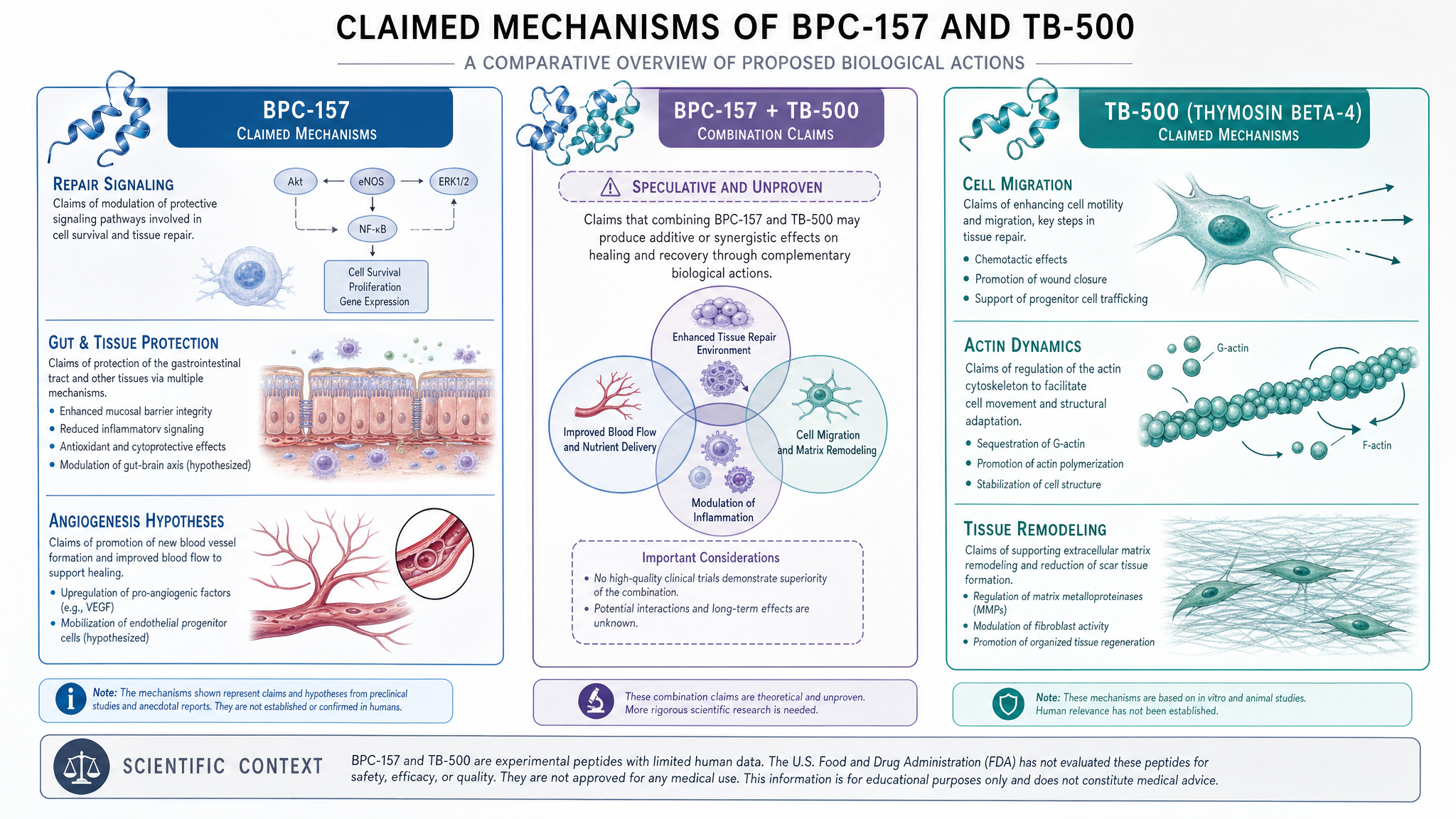
What BPC-157 is usually claimed to do
BPC-157 is commonly discussed as a repair-oriented synthetic peptide. Online claims often focus on tendons, ligaments, muscle injury, wounds, gut lining, inflammation, and general recovery. The more cautious version is that BPC-157 has been studied in many preclinical models involving tissue injury and protective signaling, but human evidence for popular uses remains limited.
The mechanisms usually discussed include:
- angiogenesis and blood-vessel-related repair signaling
- interactions with nitric oxide pathways
- tendon, ligament, and muscle injury models
- gastric and intestinal protection models
- inflammation-related tissue stress models
- wound-healing and repair signaling
Those mechanisms help explain why BPC-157 became popular. They do not establish that it reliably improves human injury outcomes, and they definitely do not establish that it becomes stronger or safer when paired with TB-500.
For a broader standalone overview, see the existing PeptideBase article on what BPC-157 is and the safety-focused article on BPC-157 side effects and unknowns.
What TB-500 is usually claimed to do
TB-500 is usually discussed in relation to thymosin beta-4 biology. The strongest scientific backbone is not “TB-500 as marketed solves recovery,” but the broader literature around thymosin beta-4 and repair-related biology.
Claims around TB-500 often involve:
- cell migration
- actin dynamics
- angiogenesis
- wound-healing biology
- tissue remodeling
- soft-tissue recovery discussions
- mobility or flexibility anecdotes
The important nuance is that TB-500 and thymosin beta-4 should not be treated as identical evidence buckets. Some online claims blur that distinction because it makes the story easier to sell. A better interpretation is that TB-500 is popular partly because thymosin beta-4 research makes repair-related hypotheses feel plausible.
For more background, see what TB-500 is and the direct comparison BPC-157 vs TB-500.
Separate evidence is not the same as combination evidence
This is the central problem with BPC-157 and TB-500 combination claims: separate evidence does not automatically become combination evidence.
If Compound A has preclinical signals in one set of models, and Compound B has mechanistic or preclinical signals in another set of models, it does not automatically follow that A plus B is better, safer, synergistic, or clinically useful in humans.
Combination claims need their own evidence because combinations can create several possibilities:
- one compound could add nothing meaningful to the other
- effects could overlap rather than stack
- the outcome could depend on timing, context, tissue type, or health status
- adverse effects or uncertainties could also combine
- one mechanism could complicate interpretation of the other
- anecdotal improvement could reflect natural recovery, rehab, rest, or placebo effects
This is not being pedantic. It is how evidence works. Otherwise every plausible pairing becomes “synergy” and every forum post becomes a protocol, which is how the internet turns biology into fan fiction with footnotes.
What mechanisms are claimed to overlap?
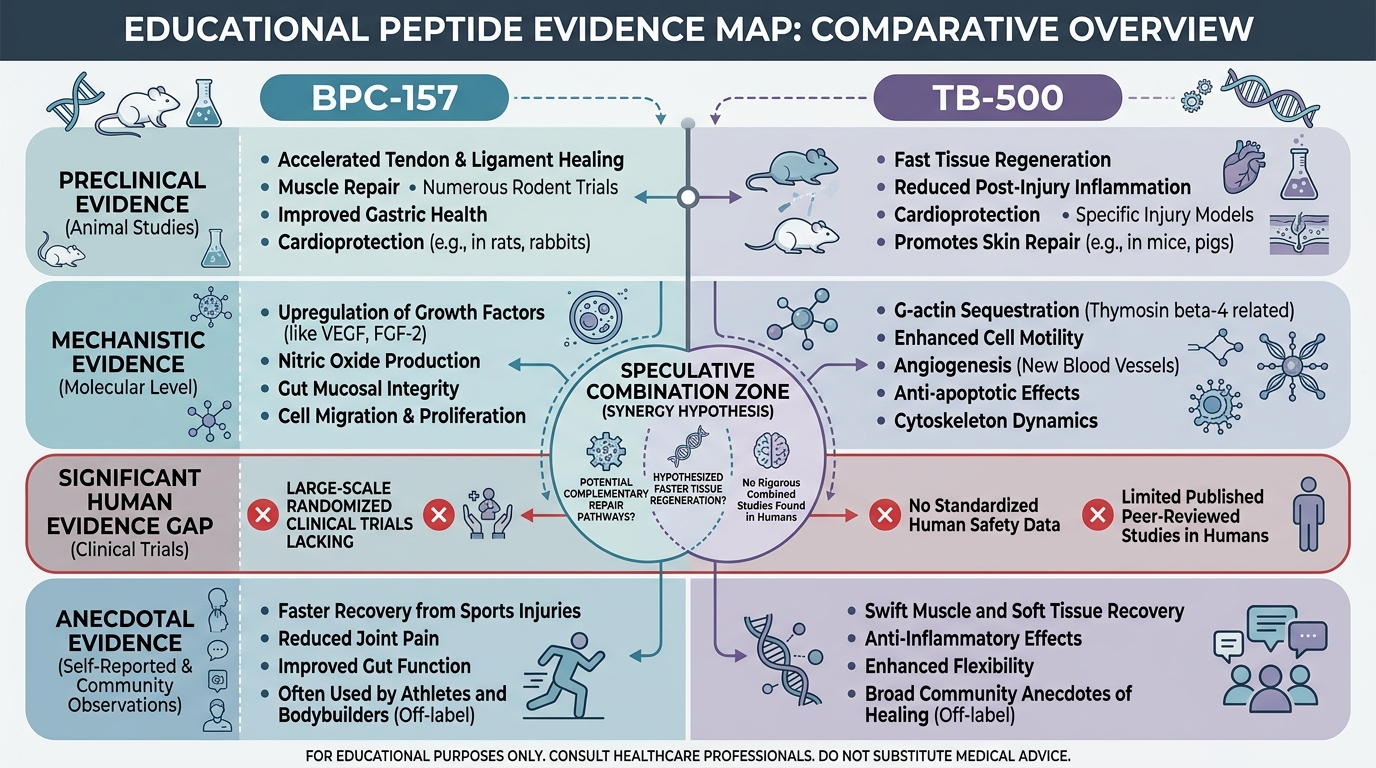
The claimed overlap usually centers on tissue repair. BPC-157 and TB-500 are both discussed around angiogenesis, wound-healing environments, inflammatory signaling, and repair coordination. That overlap is why the combination is attractive to recovery-focused readers.
A cautious mechanism map looks like this:
| Claim area | BPC-157 framing | TB-500 framing | Combination reality | |---|---|---|---| | Tissue repair | Often discussed through tendon, ligament, wound, and gut-protection models | Often discussed through thymosin beta-4 repair biology and cell movement | Plausible overlap, but combination-specific outcomes are not established | | Angiogenesis | Frequently mentioned in BPC-157 mechanism discussions | Also appears in thymosin beta-4 repair literature | Shared theme does not prove additive benefit | | Inflammation | Often framed around tissue-stress and protection models | Sometimes discussed through wound and remodeling environments | Human relevance depends on context and evidence quality | | Soft-tissue recovery | Popular online claim, mostly extrapolated | Popular online claim, often linked to repair signaling | Common claim cluster, not settled clinical proof | | Gut-related discussion | More associated with BPC-157 | Not the central TB-500 story | Pairing does not automatically strengthen gut claims |
 Mechanism overlap can explain why people ask about the combination. It cannot prove that the combination produces better human outcomes.
Mechanism overlap can explain why people ask about the combination. It cannot prove that the combination produces better human outcomes.
What evidence exists for using them together?
For the common wellness and recovery claims people search, combination-specific human evidence is not strong enough to treat BPC-157 plus TB-500 as an established approach.
Most confidence around the pair tends to come from four weaker evidence sources:
- Separate preclinical research: BPC-157 and thymosin beta-4-related studies are discussed independently, then mentally combined.
- Mechanistic plausibility: pathways such as angiogenesis, cell migration, and tissue remodeling sound complementary.
- Anecdotal reports: forums, clinics, podcasts, and social media posts describe experiences but cannot isolate cause and effect.
- Commercial framing: vendors and clinics may present combinations as obvious because bundled narratives are easier to sell.
The evidence gap is especially important because many recovery outcomes are noisy. Pain, mobility, swelling, training readiness, and injury symptoms can change because of rest, rehab, time, load management, sleep, nutrition, concurrent therapies, or expectation effects. Without controlled research, it is easy to assign the improvement to the most interesting variable.
Where online claims outrun the data
Online claims usually get too confident in five ways.
First, they treat BPC-157 and TB-500 as if both are already clinically proven for broad human recovery. That is not accurate. Each has an evidence story, but both are surrounded by uncertainty for common consumer-facing claims.
Second, they imply the combination is automatically synergistic. Synergy is not a vibe. It is something that needs evidence.
Third, they collapse different tissue problems into one category. Tendon pain, muscle strain, wound healing, gut irritation, joint discomfort, and post-training soreness are not one biological problem with one universal answer.
Fourth, they ignore safety and quality-control uncertainty. A combination can multiply unknowns, not just hoped-for benefits.
Fifth, they move from “researched pathways” to “use this for recovery” without the clinical bridge. That bridge is the part that matters.
For a broader safety framework, see Peptide Side Effects: What’s Known, What’s Unknown, and What People Overstate.
Safety and regulatory cautions
The safety discussion around BPC-157 and TB-500 together should be cautious because uncertainty exists at several levels: compound-specific effects, combination effects, product quality, route of exposure, individual health status, and regulatory status.
Important cautions include:
- Human safety evidence for popular recovery uses is limited.
- Combination-specific safety evidence is thinner than separate-compound discussion.
- Product quality, sterility, identity, and concentration can be major risks in non-approved or gray-market contexts.
- Regulatory status varies by country and use context.
- Athletic and anti-doping rules may be relevant for competitive athletes.
- Online anecdotes are not reliable safety monitoring.
This article does not provide protocols, routes, amounts, cycle lengths, sourcing advice, or personal-use recommendations. The responsible takeaway is evidence classification, not self-experimentation guidance.
How to read BPC-157 and TB-500 claims more carefully
When you see a claim about BPC-157 and TB-500 together, ask these questions:
- Is the claim based on direct combination evidence or separate evidence stitched together?
- Is the evidence human, animal, cell-based, mechanistic, or anecdotal?
- Does the claim separate BPC-157 from TB-500 and TB-500 from thymosin beta-4?
- Is the outcome specific, or does it just say “healing” and hope nobody asks questions?
- Are safety and regulatory uncertainty discussed honestly?
- Is the content trying to educate, or is it steering toward a product or protocol?
The cleaner the answer, the more useful the source. The more the claim skips straight to certainty, the more skeptical you should be.
Bottom line
BPC-157 and TB-500 are often discussed together because their repair-related mechanism stories appear to overlap. BPC-157 is usually framed around broad repair and protective signaling. TB-500 is usually framed through thymosin beta-4-related cell migration, angiogenesis, and tissue remodeling biology. That makes the combination understandable as a search topic.
But the combination is still speculative for most consumer-facing recovery claims. Separate evidence does not prove combination benefit. Mechanism does not prove outcome. Anecdote does not prove causation. And a tidy “stack” narrative can easily outrun the data.
The most evidence-aware conclusion is this: BPC-157 and TB-500 together should be understood as a popular but under-validated recovery-peptide combination claim, not as a settled, recommended, or clinically proven pairing.
FAQ
Can BPC-157 and TB-500 be used together?
This article does not provide use instructions or recommendations. The evidence-aware answer is that the combination is commonly discussed online, but strong combination-specific human evidence is limited for popular recovery claims.
Is BPC-157 better than TB-500?
Not in a broad, high-confidence way. BPC-157 and TB-500 have different mechanism stories and different reputations, but human evidence remains limited for many common recovery claims. See the dedicated BPC-157 vs TB-500 comparison for a direct breakdown.
Does combining BPC-157 and TB-500 make them work better?
That is not established. A plausible mechanism overlap does not prove additive or synergistic benefit. Combination claims need direct evidence, not just separate evidence placed side by side.
What is the evidence for BPC-157 and TB-500 together?
Most public discussion relies on separate preclinical or mechanistic evidence, broader thymosin beta-4 research, and anecdotal reports. Mature human evidence specifically validating the combination for common recovery uses is limited.
Are BPC-157 and TB-500 safe together?
Combination-specific safety evidence is limited. Safety depends on many factors, including compound identity, product quality, exposure route, individual health status, other medications or conditions, and regulatory context. This article is not medical advice.
Why do people pair BPC-157 and TB-500?
People pair them conceptually because BPC-157 is often discussed around repair and protection, while TB-500 is discussed around thymosin beta-4-related tissue remodeling and cell migration. The pairing sounds complementary, but complementary-sounding mechanisms are not the same as clinical proof.