What Is Tesamorelin? Visceral Fat Claims, Growth-Hormone Pathways, and Evidence
Evidence-aware explanation of tesamorelin, why it is searched around visceral fat and body composition, what the HIV-associated VAT evidence supports, how GH/IGF-1 pathway claims are often generalized, and where side-effect boundaries matter.
What Is Tesamorelin? Visceral Fat Claims, Growth-Hormone Pathways, and Evidence
Tesamorelin is a synthetic growth-hormone-releasing hormone analog best known for one unusually specific evidence story: reduction of excess visceral abdominal fat in adults with HIV-associated lipodystrophy. That does not mean every tesamorelin peptide claim about fat loss, body recomposition, anti-aging, or “before and after” transformation is equally supported.
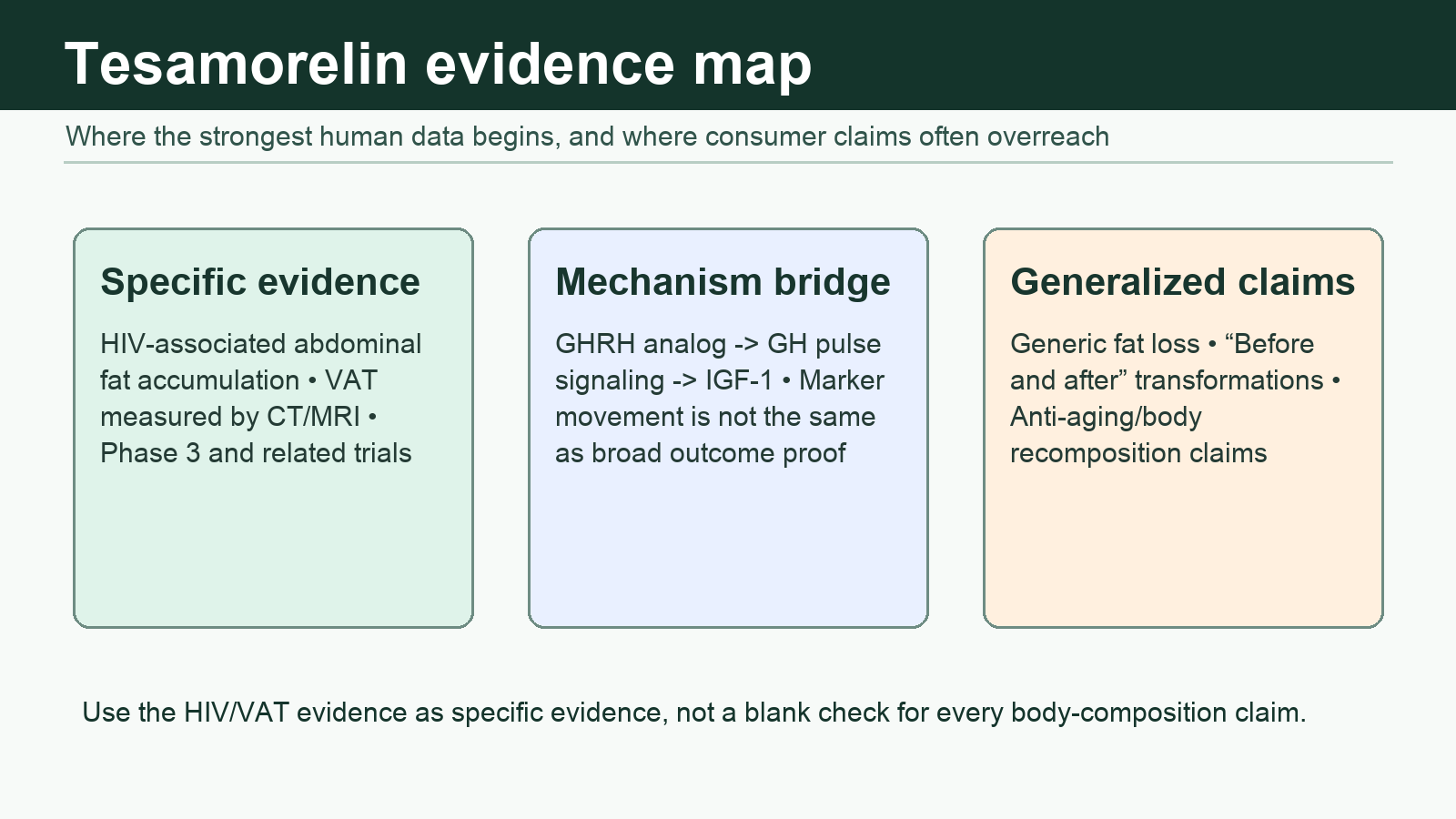
The clean way to read tesamorelin is to separate three things: what it is approved and studied for, what its growth-hormone pathway makes biologically plausible, and what online body-composition marketing often generalizes beyond the evidence.
Educational note: This article is for general peptide education only. It is not medical advice, treatment guidance, dosing guidance, sourcing guidance, purchasing guidance, or a recommendation to use tesamorelin.
Tesamorelin has a more specific evidence base than many “fat loss peptide” discussions imply. The key is not just whether visceral fat changed, but in whom, under what study conditions, and for which endpoint.
Quick Facts About Tesamorelin
Tesamorelin is a GHRH analog. It acts upstream in the growth-hormone axis by stimulating growth hormone release, which can raise downstream IGF-1.
Its strongest clinical evidence is specific. The best-supported endpoint is visceral adipose tissue reduction in adults with HIV-associated abdominal fat accumulation, not broad consumer weight loss.
It is searched like a body-composition peptide. Queries such as “tesamorelin before and after,” “tesamorelin peptide,” and “tesamorelin vs ipamorelin” usually come from people trying to understand whether the HIV/VAT evidence generalizes to non-HIV body recomposition.
It is not a simple weight-loss drug. In FDA-label trial data, VAT and waist measures changed while total body weight changed little. That distinction matters.
Safety is not trivial. Label concerns include IGF-1 elevation, fluid retention symptoms, glucose intolerance or diabetes risk, hypersensitivity, malignancy-related cautions, and pregnancy contraindication.
What Is Tesamorelin?
Tesamorelin is a synthetic analog of growth-hormone-releasing hormone, usually abbreviated GHRH. In plain English, it is designed to signal the pituitary gland to release more growth hormone in a regulated, upstream way rather than replacing growth hormone directly.
The compound is best known under the Egrifta brand family. Current U.S. labeling describes tesamorelin as indicated for reducing excess abdominal fat in adults with HIV and lipodystrophy. The FDA label also makes clear that different Egrifta formulations are not automatically interchangeable and that safety monitoring is part of the prescribing framework.
For PeptideBase readers, the important point is the category: tesamorelin sits in the growth-hormone pathway discussion, alongside compounds people compare with sermorelin, CJC-1295, and ipamorelin. But tesamorelin is not just another generic “GH peptide.” It has specific drug-label and trial history around HIV-associated visceral adiposity.
Answer block: What is tesamorelin?
Tesamorelin is a GHRH analog that stimulates growth-hormone signaling and is best known for FDA-labeled use related to excess abdominal fat in adults with HIV-associated lipodystrophy. Its evidence should not be automatically generalized to ordinary fat loss or cosmetic body recomposition.
Why Tesamorelin Is Searched Around Visceral Fat
Tesamorelin is searched around visceral fat because controlled trials measured visceral adipose tissue directly and found reductions in the studied HIV lipodystrophy population. That is more concrete than the vague “burns fat” language used around many peptides.
Visceral fat is the deeper abdominal fat around internal organs. It is different from subcutaneous fat, which sits under the skin. Many “before and after” photos mostly show visible changes in subcutaneous fat, posture, lighting, muscle tone, and water retention. Tesamorelin’s clinical story is not built on mirror photos; it is built on imaging-measured VAT in a specific medical population.
In DailyMed labeling for Egrifta, two 26-week studies in adults with HIV, lipodystrophy, and excess abdominal fat showed mean VAT reductions from baseline in the tesamorelin groups compared with placebo. The label reports mean VAT percentage changes of about -18% and -14% in the two main studies, while placebo groups changed little or increased slightly. Waist circumference moved modestly, and weight did not change much.
That pattern is the article’s central evidence boundary: tesamorelin may affect fat distribution in the studied context, but it should not be described as a universal weight-loss solution.
How Tesamorelin Works in the GH and IGF-1 Pathway
Tesamorelin works by stimulating the GHRH receptor pathway, which can increase growth hormone secretion and downstream IGF-1. That pathway is one reason people connect it to body composition, lipolysis, and “growth hormone peptide” searches.
The pathway is not magic. GHRH signaling can change endocrine markers, and those markers can relate to metabolism and body composition. But a pathway explanation is not the same as proof that a peptide produces a specific outcome in every user group.
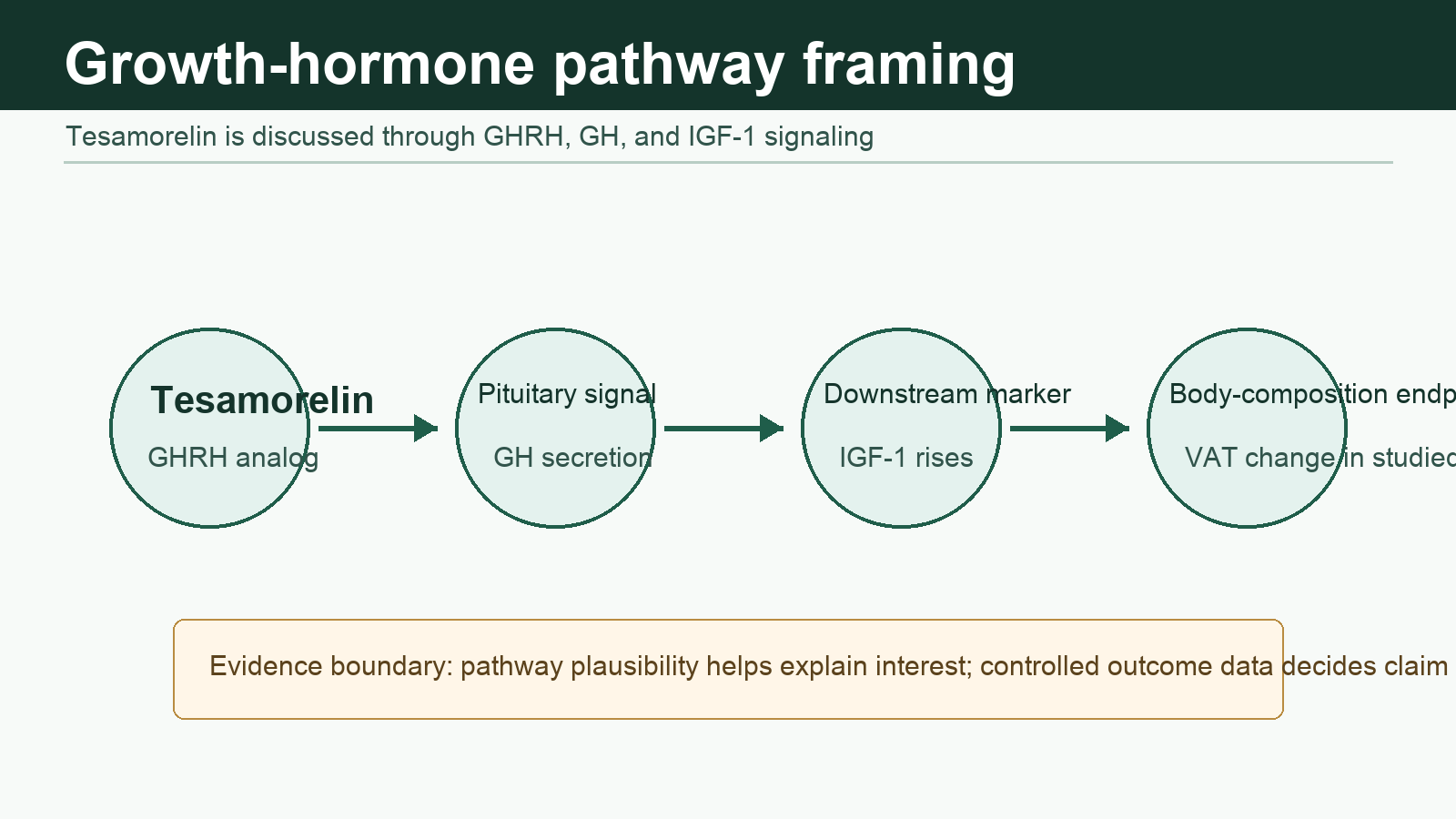
Tesamorelin is usually discussed through GH and IGF-1 signaling. The outcome claim still depends on direct human evidence for the population and endpoint being discussed.
FDA labeling explicitly notes that tesamorelin stimulates GH production and increases serum IGF-1, and that the effects of prolonged IGF-1 elevations are unknown. That is a useful built-in caution: if a peptide works through a powerful endocrine pathway, the upside claims and the safety questions travel together.
What the Evidence Shows Most Clearly
The clearest evidence for tesamorelin is not “fat loss” in the generic fitness sense. It is visceral adipose tissue reduction in adults with HIV-associated abdominal fat accumulation.
The key evidence categories are:
| Evidence area | What it supports | What it does not automatically prove | |---|---|---| | Phase 3 HIV lipodystrophy trials | VAT reduction over months in the studied population | General cosmetic fat loss in people without HIV lipodystrophy | | FDA/DailyMed labeling | Labeled indication, safety warnings, adverse reactions, and trial endpoints | Wellness, anti-aging, or off-label body-recomposition claims | | Smaller liver-fat studies in HIV | Possible effects on liver fat and metabolic markers in selected HIV populations | Broad NAFLD treatment claims for the general population | | Mechanism studies and GH-axis logic | Why tesamorelin could affect body composition biology | Guaranteed “before and after” outcomes |
A randomized clinical trial in HIV-infected adults with abdominal fat accumulation found that tesamorelin reduced visceral adipose tissue and liver fat over six months compared with placebo. That study is useful because it looked beyond appearance and used imaging-based endpoints. It is still population-specific and not a license to market tesamorelin as a general liver-fat or weight-loss treatment.
A pooled analysis of two phase 3 studies included more than 800 antiretroviral-treated adults with HIV and excess abdominal fat. That is a stronger evidence base than many research-peptide topics have. But the strength applies to that studied context, not every online use case.
Answer block: Does tesamorelin reduce visceral fat?
In controlled studies of adults with HIV-associated abdominal fat accumulation, tesamorelin reduced imaging-measured visceral adipose tissue compared with placebo. The stronger claim is specific to that population and endpoint; it should not be restated as a universal fat-loss claim.
What Gets Overgeneralized Online
The most common online mistake is turning a specific VAT finding into a broad body-transformation promise. Tesamorelin is easy to overmarket because “visceral fat” sounds precise, “growth hormone” sounds powerful, and “before and after” searches reward dramatic narratives.
The weaker claims usually look like this:
- Tesamorelin “targets belly fat” in anyone.
- Tesamorelin “melts visceral fat” without context.
- Tesamorelin produces predictable before-and-after changes.
- Tesamorelin is interchangeable with any GH secretagogue.
- Tesamorelin plus another peptide has proven synergistic body-composition effects.
The more defensible version is narrower: tesamorelin has controlled human evidence for reducing VAT in adults with HIV-associated lipodystrophy, and its endocrine mechanism explains why body-composition questions exist. Anything beyond that needs its own evidence.
This is the same evidence logic PeptideBase applies in broader guides like peptide therapy explained, CJC-1295, and peptide side effects: the exact compound, exact population, exact endpoint, and exact claim all matter.
Tesamorelin Before and After: What Photos Can and Cannot Tell You
“Tesamorelin before and after” is a high-interest search, but photos are weak evidence by themselves. Lighting, hydration, training, diet, posture, camera angle, and concurrent medications can all change appearance.
The more reliable question is whether a study measured visceral fat with imaging and controlled the comparison. Tesamorelin’s best evidence comes from that kind of structure, not from photo anecdotes.
That does not make anecdotes worthless. They can reveal what people care about, what side effects show up in real life, and what expectations are circulating. They just cannot prove cause, dose-response, safety, or generalizability.
Answer block: Are tesamorelin before-and-after results reliable?
Before-and-after photos can be interesting, but they are not reliable evidence that tesamorelin caused a specific fat-loss result. Imaging-based VAT studies are much stronger, especially when placebo comparison and population details are clear.
Tesamorelin vs Ipamorelin and CJC-1295
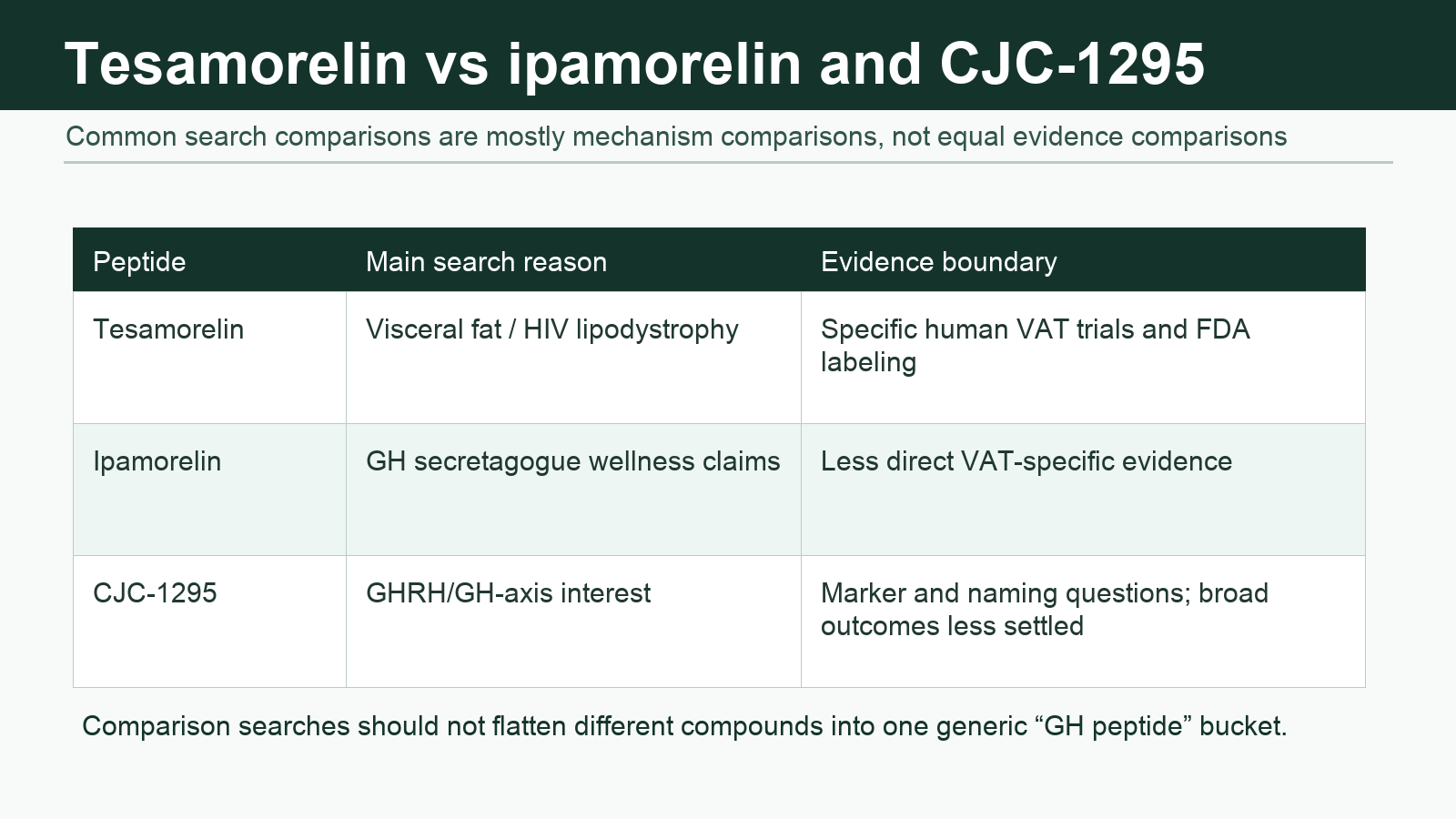
Tesamorelin vs ipamorelin is a common comparison because both are discussed around growth-hormone signaling. The comparison is useful, but only if it does not flatten different mechanisms and evidence bases into one “GH peptide” bucket.
Tesamorelin is a GHRH analog. Ipamorelin is commonly discussed as a growth-hormone secretagogue/ghrelin-receptor pathway peptide. CJC-1295 is also tied to GHRH signaling, but its marketplace naming and evidence questions are different. That means the comparison should focus on mechanism category, evidence specificity, and claim boundaries.
Tesamorelin comparisons are most useful when they separate mechanism from evidence. Similar pathway language does not mean identical clinical support.
| Comparison | Better framing | |---|---| | Tesamorelin vs ipamorelin | Tesamorelin has specific VAT trial and label history; ipamorelin is usually discussed more broadly around GH secretagogue interest. | | Tesamorelin vs CJC-1295 | Both sit near GHRH/GH-axis discussions, but CJC-1295 has different naming, pharmacology, and evidence-boundary issues. | | Tesamorelin vs sermorelin | Both are GHRH-pathway peptides, but search intent differs: sermorelin is often framed around GH deficiency or wellness clinics, while tesamorelin is strongly associated with HIV lipodystrophy VAT data. |
For more cluster context, see sermorelin vs ipamorelin and CJC-1295.
Side Effects and Safety Boundaries
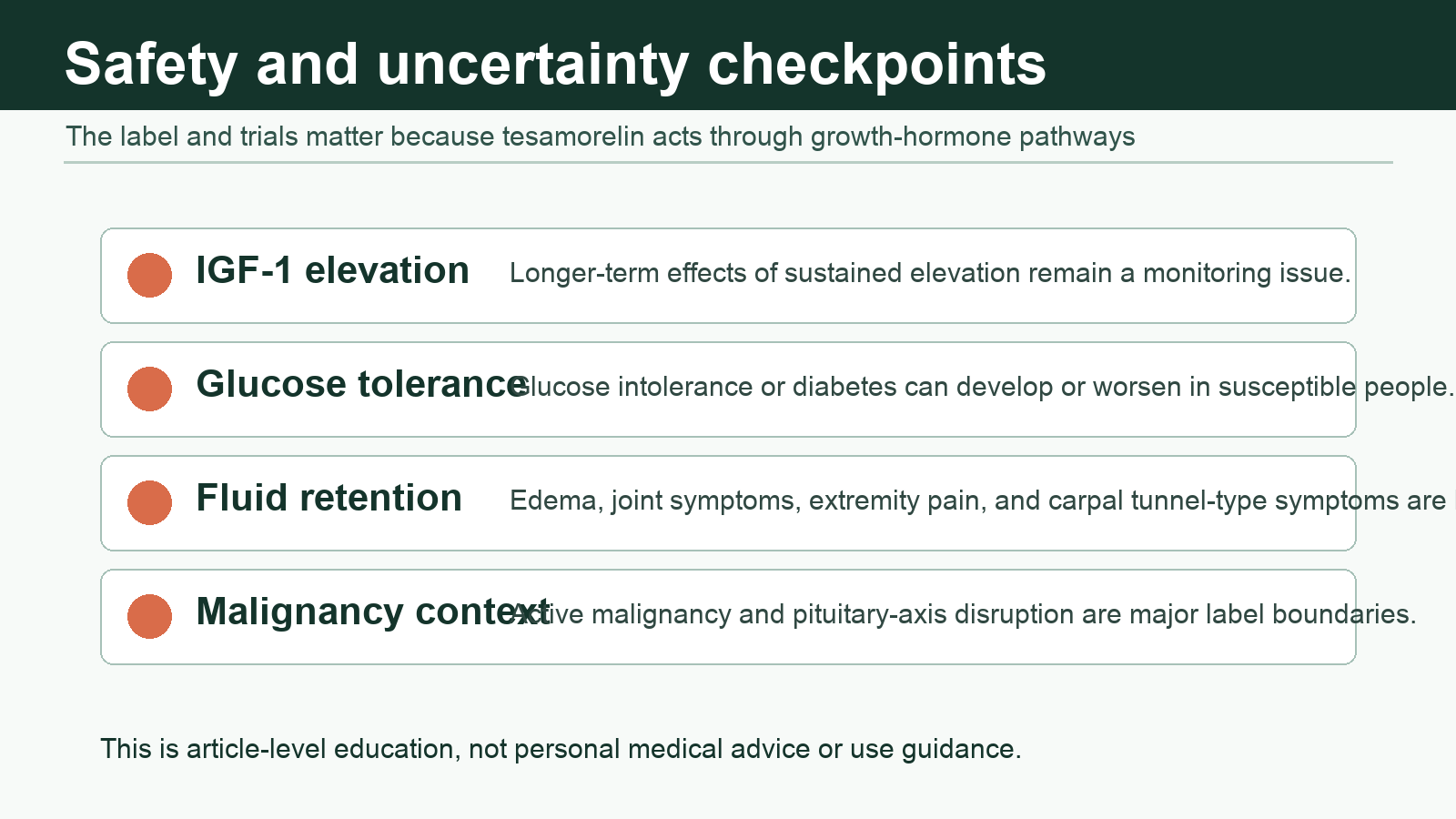
Tesamorelin side effects matter because the peptide acts through the growth-hormone axis. The same pathway that makes body-composition claims plausible also creates monitoring and risk questions.
Current FDA labeling lists common adverse reactions including joint pain, injection-site erythema and itching, pain in extremity, peripheral edema, and muscle pain. The label also highlights warnings and precautions around malignancy risk context, elevated IGF-1, fluid retention, glucose intolerance or diabetes mellitus, hypersensitivity reactions, and acute critical illness.
The safety question is not just “does it work?” It is whether GH/IGF-1 pathway effects are appropriate and monitored in the person and context being discussed.
Important safety boundaries include:
- IGF-1 elevation: Tesamorelin can raise IGF-1, and prolonged elevations are an uncertainty in the label.
- Glucose concerns: Glucose intolerance or diabetes can develop; people with diabetes may require monitoring for worsening complications.
- Fluid-retention symptoms: Edema, joint pain, extremity pain, and carpal tunnel-type symptoms are part of the known risk conversation.
- Malignancy context: Active malignancy is a major label contraindication, and recurrent malignancy is a discontinuation concern in labeling.
- Pregnancy: Pregnancy is listed as a contraindication in the label.
None of this means tesamorelin is “bad.” It means the safety profile is not compatible with casual, unsupervised marketing language. A real evidence-aware article has to keep the benefit and risk story in the same frame.
Answer block: What are tesamorelin side effects?
Label-discussed tesamorelin risks include injection-site reactions, joint or muscle symptoms, extremity pain, peripheral edema, fluid retention, carpal tunnel-type symptoms, IGF-1 elevation, glucose intolerance or diabetes risk, hypersensitivity, and malignancy-related cautions.
Evidence Boundaries: What Is Specific vs Generalized
The most important distinction is specific evidence versus generalized inference.
Specific evidence means a claim is tied to tesamorelin itself, measured in humans, in a defined population, against a comparison group, using a relevant endpoint. Generalized inference means the claim is extrapolated from mechanism, related peptides, anecdotes, or body-composition theory.
For tesamorelin, the specific evidence is strongest around:
- HIV-associated abdominal fat accumulation.
- Imaging-measured visceral adipose tissue.
- GH/IGF-1 pathway marker changes.
- Label-defined safety and adverse-reaction monitoring.
The generalized or weaker evidence areas include:
- Non-HIV cosmetic belly-fat use.
- Predictable “before and after” transformation claims.
- Broad anti-aging or longevity claims.
- Tesamorelin combinations with ipamorelin, CJC-1295, GLP-1 drugs, or other compounds.
- Claims that visceral fat loss will automatically translate into broad metabolic benefit for every population.
This boundary is not academic nitpicking. It is the difference between education and marketing with a lab coat on.
Who Should Be Especially Cautious
People should be especially cautious about tesamorelin claims when the discussion involves cancer history, pituitary-axis disruption, pregnancy, diabetes or glucose intolerance, retinopathy risk, edema, carpal tunnel symptoms, critical illness, or multiple endocrine-active compounds.
This article is not evaluating individual suitability. The point is simpler: tesamorelin is not just a lifestyle supplement topic. It has drug-label warnings, endocrine effects, and specific studied populations. Any content that skips those details is giving readers a cleaner story than the evidence supports.
How to Read Tesamorelin Claims Online
The fastest way to evaluate a tesamorelin claim is to ask what kind of evidence the claim is actually leaning on.
Use this filter:
- Is the claim about HIV-associated visceral adiposity or general fat loss?
- Was visceral fat measured with imaging, or inferred from appearance?
- Is the claim based on tesamorelin specifically, or another GH-axis peptide?
- Does the source discuss IGF-1, glucose, fluid retention, and label cautions?
- Is the page giving dosing, sourcing, or purchasing advice instead of evidence boundaries?
If the answer keeps drifting toward vague transformation language, the claim probably needs downgrading.
FAQ
Is tesamorelin a peptide?
Yes. Tesamorelin is a synthetic peptide analog of growth-hormone-releasing hormone. It is often searched as “tesamorelin peptide,” but the medically relevant details are its GHRH pathway, labeled indication, evidence base, and safety warnings.
Is tesamorelin approved for visceral fat?
Tesamorelin is FDA-labeled for reducing excess abdominal fat in adults with HIV and lipodystrophy. That is more specific than saying it is approved for general visceral fat reduction in anyone.
Does tesamorelin cause weight loss?
Tesamorelin should not be described as a simple weight-loss drug. In label trial data, visceral adipose tissue and waist measurements changed while total weight changed little. The better framing is fat-distribution evidence in a specific studied population.
Is tesamorelin better than ipamorelin?
“Better” depends on the claim. Tesamorelin has more specific clinical evidence around HIV-associated VAT reduction. Ipamorelin is usually discussed in a broader GH-secretagogue context, where claims often rely more on mechanism and less on tesamorelin-like VAT endpoint data.
What should readers be skeptical of?
Be skeptical of guaranteed before-and-after claims, universal belly-fat claims, protocol-heavy pages, commercial claims, and comparisons that treat tesamorelin, CJC-1295, sermorelin, and ipamorelin as interchangeable because they all touch growth-hormone signaling.
Bottom Line
Tesamorelin is one of the more evidence-specific peptides in the body-composition conversation, but that specificity is exactly why it should be handled carefully. The best-supported story is not generic fat loss. It is imaging-measured visceral fat reduction in adults with HIV-associated abdominal fat accumulation, with GH/IGF-1 pathway effects and label-level safety cautions.
The strongest tesamorelin article is not the one that sounds most dramatic. It is the one that keeps the exact claim attached to the exact evidence.
Sources
- FDA prescribing information for Egrifta WR, revised March 2025
- DailyMed Egrifta WR prescribing information
- Falutz et al., randomized placebo-controlled tesamorelin trial in HIV-associated abdominal fat accumulation
- Falutz et al., pooled analysis of two phase 3 tesamorelin trials
- Stanley et al., tesamorelin effects on visceral fat and liver fat in HIV-infected adults
- Efficacy and safety of tesamorelin in people with HIV on integrase inhibitors